Pharmacology: Pharmacodynamics: Mechanism of action: Zoledronic acid is a highly potent drug that belongs to the bisphosphonates class of drugs, which act primarily on bone. It is one of the most potent inhibitors of osteoclastic bone resorption known to date.The selective action of bisphosphonates on bone is based on their high affinity for mineralised bone, but the precise molecular mechanism leading to the inhibition of osteoclastic activity is still unclear. In long-term animal studies, zoledronic acid inhibits bone resorption without adversely affecting the formation, mineralization or mechanical properties of bone.
In addition to being a very potent inhibitor of bone resorption, zoledronic acid also possesses several anti-tumour properties that could contribute to its overall efficacy in the treatment of metastatic bone disease. The following properties have been demonstrated in preclinical studies:
In vivo: Inhibition of osteoclastic bone resorption, which alters the bone marrow microenvironment making it less conducive to tumour cell growth, anti-angiogenic activity, anti-pain activity.
In vitro: inhibition of osteoblast proliferation, direct cytostatic and pro-apoptotic activity on tumour cells, synergistic cytostatic effect with other anti-cancer drugs, antiadhesion/invasion activity.
Clinical Studies: Clinical trial results in the treatment of osteolytic, osteoblastic and mixed bone metastases and osteolytic lesions of multiple myeloma, in conjunction with standard antineoplastic therapy: Zoledronic acid was compared to placebo for the prevention of skeletal related events (SREs) in adult prostate cancer patients with 214 men receiving Zoledronic acid 4 mg versus 208 receiving placebo. After the initial 15 months of treatment, 186 patients continued for up to an additional 9 months, giving a total duration of double-blind therapy up to 24 months. Zoledronic acid 4 mg demonstrated a significant advantage over placebo for the proportion of patients experiencing at least one skeletal related event (SRE) (38% for Zoledronic acid 4 mg versus 49% for placebo, p=0.028), delayed the median time to first SRE (488 days for Zoledronic acid 4 mg versus 321 daysfor placebo, p=0.009), and reduced the annual incidence of event per patient - skeletal morbidity rate (0.77 for Zoledronic acid 4 mg versus 1.47 for placebo, p=0.005). Multiple event analysis showed 36% risk reduction in developing skeletal related events in the Zoledronic acid group compared with placebo (p=0.002). Pain was measured at baseline and periodically throughout the trial. Patients receiving Zoledronic acid reported less increase in pain than those receiving placebo, and the differences reached significance at months 3, 9, 21 and 24. Fewer Zoledronic acid patients suffered pathological fractures. The treatment effects were less pronounced in patients with blastic lesions. Efficacy results are provided in Table 1.
In a second study, Zoledronic acid reduced the number of SREs and extended the median time to an SRE by over two months in the population of adult patients who had other solid tumors involving bone, which had a median survival of only six months (134 patients with non-small-cell lung cancer [NSCLC], 123 with other solid tumors treated with Zoledronic acid vs 130 patients with NSCLC, 120 with other solid tumors treated with placebo). After initial 9 months of treatment, 101 patients entered the 12 month extension study, and 26 completed the full 21 months. Zoledronic acid 4 mg reduced the proportion of patients with SREs (39% for Zoledronic acid 4 mg versus 48% for placebo, p=0.039), delayed the median time to first SRE (236 days for Zoledronic acid 4 mg versus 155 days for placebo, p=0.009), and reduced the annual incidence of events per patient - skeletal morbidity rate (1.74 for Zoledronic acid 4 mg versus 2.71 for placebo, p=0.012). Multiple event analysis showed 30.7% risk reduction in developing skeletal related events in the Zoledronic acid group compared with placebo (p=0.003). The treatment effect in non-small cell lung cancer patients appeared to be smaller than in patients with other solid tumors. Efficacy results are provided in Table 2. (See Tables 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
In a third phase III randomized, double-blind trial comparing Zoledronic acid 4 mg to pamidronate 90 mg, 1,122 adult patients (564 Zoledronic acid 4 mg, 558 pamidronate 90 mg) with multiple myeloma or breast cancer with at least one bone lesion were treated with 4 mg Zoledronic acid or 90 mg pamidronate every 3 to 4 weeks. Eight patients were excluded from the efficacy analysis because of good clinical practice non-compliance. 606 patients entered the 12-month, double-blind extension phase. Total therapy lasted up to 24 months. The results demonstrated that Zoledronic acid 4 mg showed comparable efficacy to 90 mg pamidronate in the prevention of skeletal related events. The multiple event analyses revealed a significant risk reduction of 16% (p=0.030) in patients treated with Zoledronic acid 4 mg. Efficacy results are provided in Table 3.
Click on icon to see table/diagram/image
In clinical trials performed in adult patients with bone metastases or osteolytic lesions, the overall safety profile amongst all treatment groups (zoledronic acid 4 mg, and pamidronate 90 mg and placebo) was similar in types and severity.
Zoledronic acid was also studied in a double-blind, randomized, placebo-controlled trial in 228 adult patients with documented bone metastases from breast cancer to evaluate the effect of Zoledronic acid on the skeletal related event (SRE) rate ratio, calculated as the total number of SRE events (excluding hypercalcaemia and adjusted for prior fracture), divided by the total risk period. Patients received either 4 mg Zoledronic acid or placebo every four weeks for one year. Patients were evenly distributed between Zoledronic acid-treated and placebo groups.
The SRE rate ratio at one year was 0.61, indicating that treatment with Zoledronic acid reduced the rate of occurrence of SREs by 39% compared with placebo (p=0.027). The proportion of patients with at least one SRE (excluding hypercalcaemia) was 29.8% in the Zoledronic acid-treated group versus 49.6% in the placebo group (p=0.003). Median time to onset of the first SRE was not reached in the Zoledronic acid-treated arm at the end of the study and was significantly prolonged compared to placebo (p=0.007). Zoledronic acid reduced the risk of SREs by 41% in a multiple event analysis (risk ratio=0.59, p=0.019) compared with placebo.
In the Zoledronic acid-treated group, decreases in pain scores from baseline (using the Brief Pain Inventory, BPI) occurred from 4 weeks onwards and at every subsequent time point during the study, while the pain score in the placebo group remained unchanged or increased from baseline (figure). Zoledronic acid inhibited the worsening of the analgesic score more than placebo. In addition, 71.8% of Zoledronic acid-treated patients versus 63.1% of placebo patients showed improvement or no change in the ECOG performance score at the final observation. (See figure.)
Click on icon to see table/diagram/image
Clinical trial results in the treatment of HCM: Clinical studies in hypercalcaemia of malignancy (HCM) demonstrated that the effect of zoledronic acid is characterized by decreases in serum calcium and urinary calcium excretion.
To assess the effects of Zoledronic acid versus pamidronate 90 mg, the results of two pivotal multicentre studies in adult patients with HCM were combined in a pre-planned analysis. The results showed that Zoledronic acid 4 mg and 8 mg were statistically superior to pamidronate 90 mg for the proportion of complete responders at day 7 and day 10. There was faster normalization of corrected serum calcium at day 4 for Zoledronic acid 8 mg and at day 7 for Zoledronic acid 4 mg and 8 mg. The following response rates were observed Table 4:
Click on icon to see table/diagram/image
Median time to normocalcaemia was 4 days. By day 10 the response rate was 87 to 88 % for the Zoledronic acid treatment groups versus 70 % for pamidronate 90 mg. Median time to relapse (re- increase of albumin-corrected serum calcium ≥ 2.9 mmol/L) was 30 to 40 days for patients treated with Zoledronic acid versus 17 days for those treated with pamidronate 90 mg. The results showed that both Zoledronic acid doses were statistically superior to pamidronate 90 mg for time to relapse. There were no statistically significant differences between the two Zoledronic acid doses.In clinical trials performed in adult patients with hypercalcaemia of malignancy (HCM), the overall safety profile amongst all three treatment groups (zoledronic acid 4 and 8 mg and pamidronate 90 mg) was similar in types and severity.
Pharmacokinetics: Single and multiple 5- and 15-minute infusions of 2, 4, 8 and 16 mg zoledronic acid in 64 patients with bone metastases yielded the following pharmacokinetic data.
No pharmacokinetic data for zoledronic acid are available in patients with hypercalcemia. After initiating the infusion of zoledronic acid, the plasma concentrations of drug rapidly increased, achieving their peak at the end of the infusion period, followed by a rapid decline to <10% of peak after 4 hours and < 1% of peak after 24 hours, with a subsequent prolonged period of very low concentrations not exceeding 0.1% of peak prior to the second infusion of drug on day 28.
Distribution: Zoledronic acid shows low affinity for the cellular components of human blood, with a mean blood to plasma concentration ratio of 0.59 in a concentration range of 30 ng/mL to 5000 ng/mL The plasma protein binding is low, with the unbound fraction ranging from 60% at 2 ng/mL to 77% at 2000 ng/mL of zoledronic acid.
Biotransformation/Metabolism: Zoledronic acid is not metabolised and is excreted unchanged via the kidney. Zoledronic acid does not inhibit human P450 enzymes
in vitro.
Elimination: Intravenously administered zoledronic acid is eliminated via a triphasic process: rapid biphasic disappearance from the systemic circulation, with half-lives of t
½ alpha 0.24 and t
½ beta 1.87 hours, followed by a long elimination phase with a terminal elimination half-life of t
½ gamma 146 hours. There was no accumulation of drug in plasma after multiple doses of the drug given every 28 days. Over the first 24 hours, 39 ± 16% of the administered dose is recovered in the urine, while the remainder is principally bound to bone tissue. From the bone tissue it is released very slowly back into the systemic circulation and eliminated via thekidney. The total body clearance is 5.04 ± 2.5 L/h, independent of dose, and unaffected by gender, age, race, and body weight.
Linearity/Non-linearity: The zoledronic acid pharmacokinetics were found to be dose independent. Increasing the infusion time from 5 to 15 minutes caused a 30% decrease in zoledronic acid concentration at the end of the infusion, but had no effect on the area under the plasma concentration versus time curve.
Special populations: Hepatic impairment: No pharmacokinetic data for zoledronic acid are available in patients with hepatic impairment. Zoledronic acid does not inhibit human P450 enzymes
in vitro, shows no biotransformation and in animal studies <3% of the administered dose was recovered in the feces, suggesting no relevant role of liver function in the pharmacokinetics of zoledronic acid.
Renal impairment: The renal clearance of zoledronic acid was correlated with creatinine clearance, renal clearance representing 75 ± 33% of the creatinine clearance, which showed a mean of 84 ± 29 mL/min (range 22 to 143 mL/min) in the 64 cancer patients studied. Population analysis showed that for a patient with creatinine clearance of 50 mL/min (moderate impairment), the corresponding predicted clearance of zoledronic acid would be 72% of that of a patient showing creatinine clearance of 84 mL/min. Only limited pharmacokinetic data are available in patients with severe renal insufficiency (creatinine clearance <30 mL/min). The use of Zoledronic acid is not recommended in patients with severe renal impairment (see Precautions).
Effect of gender, age and race: The three pharmacokinetic studies conducted in cancer patients with bone metastases reveal no effect by gender, race, age (range 38 to 84 years), and body weight on zoledronic acid total clearance.
Toxicology: Non-Clinical Safety Data: Toxicity studies: In the bolus parenteral studies, Zoledronic acid was well tolerated when administered subcutaneously to rats and intravenously to dogs at doses up to 0.02 mg/kg daily for 4 weeks. Administration of 0.001 mg/kg/day subcutaneously in rats and 0.005 mg/kg intravenously once every 2 to 3 days in dogs for up to 52 weeks was also well tolerated.
The most frequent finding in the repeat-dose studies consisted of increased primary spongiosa in the metaphysis of long bones in growing animals at nearly all doses, a finding that reflected the compound's pharmacological antiresorptive activity.
The kidney was identified as a major target organ for toxicity in parenteral studies with zoledronic acid. In the intravenous infusion studies, renal tolerability was observed in rats given six infusions at doses of up to 0.6 mg/kg at 3-day intervals, while five infusions of 0.25 mg/kg administered at 3-week intervals were well tolerated in dogs.
Reproduction toxicity: Teratogenicity studies were performed in two species, both via subcutaneous administration of zoledronic acid. Teratogenicity was observed in the rat at doses ≥0.2 mg/kg/day and was manifested by external, visceral and skeletal malformations. Dystocia was observed at the lowest dose (0.01 mg/kg/day) tested in rats.
No teratogenic or embryo/fetal effects were observed in the rabbit, although maternal toxicity was marked at 0.1 mg/kg/day. Adverse maternal effects were associated with, and may have been caused by, drug-induced hypocalcaemia.
Mutagenicity: Zoledronic acid was not mutagenic
in vitro and
in vivo in the mutagenicity tests performed.
Carcinogenicity: In oral carcinogenicity studies in rodents, zoledronic acid revealed no carcinogenic potential.



 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image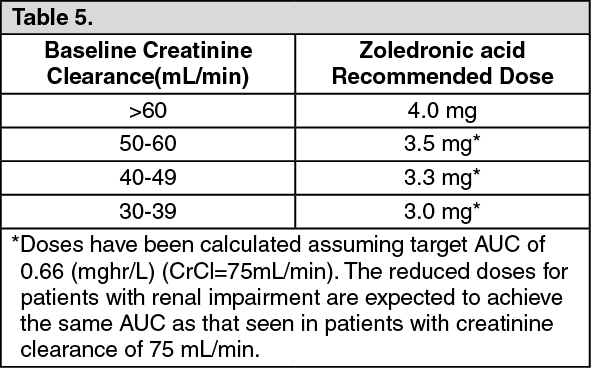 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image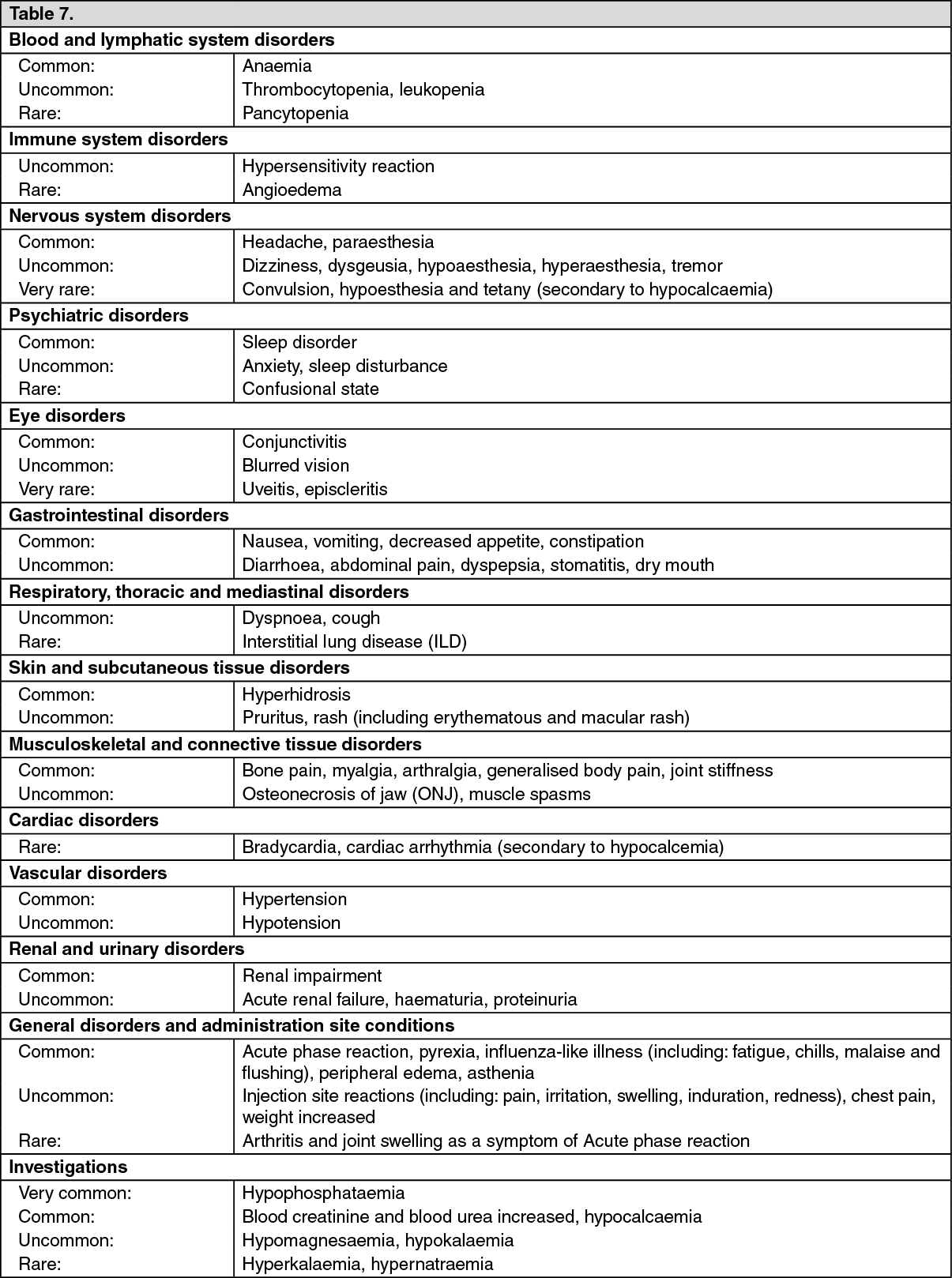 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out
